

- Introduction
This Blog is based on my experience as a unpaid care giver. My intention is to raise discussion about the way ND people access public services, rather than focus too much on my experiences. Indeed, I see parallels between my experiences looking after an aging parent and those of parents supporting ND children through school.
In 2014 my mother at the age of 85, was taken seriously ill. She had a perforated ulcer. After 4 months she was discharged from hospital but was no longer able to live independently.
Her preference was to live in her own home. I therefore made a largely pragmatic decision to move to her house in order to support her. I was then able to rent out the place I had been living to offset some lost income. During the 9-year period we have mostly needed support from live in carers due to my mother’s high fall risk. She had a minor stroke while in Hospital which has impacted on her balance.
When I talk to people of my age, around 60, it is clear, the overwhelming majority of us, have experience of supporting aging family members. It is also clear, there is no right way to do this. Nothing will ever feel perfect. The choices I have made have only been possible as I had quite a high degree of financial security and my mother owns a house in the South of England.
I have not fully referenced this article as so much of it relates to my personal experience. I am happy to provide additional material if required.
- ND people are on average more likely to become unpaid care givers than non-ND people.
Many ND conditions run in families. It is therefore more likely that ND parents will have ND children. There children may therefore need extra support. I am not aware of any evidence that parents of ND children will necessarily have additional care needs. (Kirby, 2021)
People in less stable employment are more likely to pick up care responsibilities (for children or parents.) I was first made aware of this phenomenon in a discussion about women entrepreneurship led by Carol Ekinsmyth of The University of Portsmouth (Ekinsmyth, 2013). In the discussion it was pointed out women frequently set up businesses, in order, to combine work with care responsibilities, while their partner progresses their career.
The argument being families collectively make rational decisions. It therefore makes sense, that the person in the most stable employment should focus on work and the other partner should take lead responsibility for providing care. Historically men have tended to be the more stable earners but over the past 50 years the gap has narrowed markedly. The trend in care giving has followed this pattern. Women are more likely to be care givers than men, but the gap is narrowing.
ND people are more likely to be in less stable employment than non ND people. (See our post on employment (Freeman, 2023)). It is therefore likely that ND people will pick up care responsibility more often than other family members. Carer UK statistics seem to confirm the pattern that people in less stable employment and on lower incomes are more likely to become carers as the opportunity cost is lower. (Careruk, 2024)
- Being a caregiver can be rewarding but also has costs.
BBC Radio 4 broadcasts a long-standing series, of interviews with prominent disabled people entitled no triumph no tragedy. This is how I feel about being a care giver. I have made a series of pragmatic decisions, in the best way I can, to cope with a challenge most people of my age face. Its neither heroic nor disastrous.
Everyone is different and will perceive the role of being a care giver in a different light. I started with several advantages. I am relatively financially secure and have been able to continue with some work. My mother is well off and until recently has been able to self-fund a lot of support. I have a supportive family. My sisters are not able to directly get involved (one of my sisters lives abroad, the other over 100 miles away and has family commitments of her own). We agree on what we want to achieve and the support my mother needs. It has also been much easier to make the choice to be a carer because I am single. I have not had to manage the tension between my mothers needs and my partners or family’s needs.
When I started, I feared my time as a care giver would not last long, to my surprise I have been in the role over 9 years. The role is characterised by uncertainty, particularly my mother’s changing health. Most changes are imperceptible on a day-to-day basis. Frequently I have not noticed how my level of commitment has retched up. Only by looking back over a six month or one year period can I tell what has changed. Other changes are very sudden eg a fall or illness such as Covid. The need for constant vigilance adds to stress.
The reflections in this section, most closely relate to the period 2015 to 2020. During this period although frail and very likely to fall, my mother was in relatively good health and enjoying a good quality of life . During the covid period 2020 -2022 I felt very fortunate to be living with her. In 2021 my Mum was diagnosed with vascular dementia. The diagnosis did not make her a different person. The year before diagnosis was largely the same as the year after diagnosis. However, looking after her has gradually become more challenging as her traits have become more pronounced.
The impact of Covid was also significant. Over the two years she got used to me being around. This is making it much more difficult for me to get out. I was always going to find this period of decline hard. I am not sure that for me, managing it in a different way would work any better.
3.1) What is good.
3.1.1)- Being a care giver can be a fulfilling and meaningful activity.
Over the last nine years I have had many good times with my mother. I have got to know her better. Living with my mother, has led me to feel reassured, that she is as comfortable and safe as I can make her. In supporting her I have frequently felt I was doing something important and gained a sense of security from her being around.
3.1.2) My mental health improved after making the decision to be a care giver
Being a carer resolved a tension in my life. My mother was becoming frailer and needed more support. My sisters and I had tried to persuade her to move into sheltered accommodation or get more support at home, but she was not having it. On a Sunday evening, I would feel very bad leaving her on her own when she was clearly depressed and vulnerable. Being with her has removed this sense of guilt and anxiety. It also reduced my loneliness and the sense of being pulled in several directions at once.
3.1.3) I have been able to enjoy work (and voluntary activity more)
Because I have been lucky enough to be able to rent out my own home, I am under less pressure to earn as much from my work as was previously the case. In the reduced time I have available for work, I have been able to focus on things I find satisfying. I am very fortunate that a small group of clients have engaged me in a steady stream of interesting work. I have also been able to engage in unpaid activities, including my involvement in the ND community which has helped me understand myself better.
3.2) What is difficult.
3.2.1) Caring is Tough
In his play, The Lady in the Van , Alan Bennett declares that “caring is all about shit”. This is true. Caring undoubtedly involves doing a lot of chores, some of which are not pleasant. You also have to put up with a lot of rubbish. Getting appointments at the General Practitioners GP (Doctors Surgery) can be frustrating, waiting in all day for care professionals who don’t turn up is annoying , Spending hours in Hospital Accident and Emergency ( A & E) waiting for a fall to be checked over is stressful. Caring also involves dealing with emotional garbage. Even when faculties are failing, mothers can press buttons which provoke a reaction. Contemplating loss is not easy.
3.2.2) – Economic Cost
Although I have been able to combine care with work my income has dropped, I am also not making pension contributions. My reduced economic activity therefore has both immediate and long-term consequences. I am however earning more than £140 per week, I therefore cannot claim carers allowance. (Gov.uk , 2024) . It feels slightly strange that child benefit is a universal benefit, yet carers allowance is means tested.
3.2.3) Freedom is Restricted
Although my mother has a live in carer (her core hours are 8am to 8pm) Ensuring care is in place when I go out for an evening or have a break can be a major logistic exercise. At short notice I need to be able to attend and provide transport to appointments. With GPs and Hospitals you have to take what you given, trying to negotiate slots which fit with work or other commitments is almost impossible.
- The Social Care System is Difficult for Everyone to Navigate.
The challenges of navigating the health and social care system impact on all service users not just Neurodivergent People. Three of the issues which are currently most in my mind are outlined below but this is not an exhaustive list.
4.1) Almost all parts of the system are overstretched and underfunded.
GPs, Hospital Accident and Emergency (A&E) departments, other health teams (eg mental health and physio therapy) as well as council adult social care departments are all over stretched. This leads to delays penny pinching and poor advice.
Getting appointments is difficult and wait times can be lengthy. Our record in A&E is 18 hours. Our social care department has taken more than 9 months to sort out their contribution to my mother’s care package.
After a fall my mother at one time was reluctant to eat. A nurse proscribed a high calorie shake. When a week later we visited the GP, he was very critical. He complained how expensive the shake was , and suggested I should make my mother apple crumble and ice cream, instead as that would be just as good. Probably true but not totally helpful when you as a carer are feeling under pressure.
More seriously the pressure can lead to bad advice. The mental health service recently changed my mother’s medication. (This occurred because social services felt changing her medicine would help her sleep better as they did not wish to fund night care). The new medicine stopped my mother being able to walk. It was not a total surprise as the same medicine had the same effect 6 months earlier when proscribed by the GP, but no communication had occurred between mental health team and GP.
Inevitably the problem occurred at the weekend. I called the out of hours mental health team. They denied this was a known side effect of the medicine despite it being listed number two on list of adverse reactions, on the leaflet enclosed with the pills. They advised that we should go to A&E. I did not want to follow this advice. Taking an agitated 95 year old to A&E on a Saturday night is not for the feint hearted.
When I told my mother’s care agency, I was informed that if I did not follow the advice, social services could treat it as a safeguarding issue, if they wanted to argue I was not caring for my mother properly. Which they might choose to do as residential care is cheaper than live in home care. I was advised to call 111 (one part of the system, which from my recent experience is working well) I spoke to a Doctor at 2.30 am in the morning . He agreed she should not go to A&E and that she should come off the medicine. Her ability to walk was restored in 24 hours.
4.2) Information is Asymmetric. Professionals whose job title suggest they are advocates are also frequently budget holders and therefore have a dual role as gatekeepers.
Professionals who hold information, don’t always tell you what you need to know when you need to know it. Hording information can allow agencies to protect their budgets.
The allocation of scares resources is an inevitable focus for the health and social care system. The National Institute for Health and Care Excellence NICE, provides guidelines on how an estimate of quality adjusted life years can be used to assess if a treatment represents value for money. (NICE, 2024) This is right and proper. In my mother’s case the calculation, worked in her favour she had an expensive operation and 2 months in intensive care when she was 85. She did not have to pay a penny. She is still living 9 and half years later. For most of that period she has had a good quality of life. Probably as a panicking carer waiting for the anaesthetist to explain what was going on I should not have been thinking about health economics.
For me as a care giver the way the social care system works has been less transparent and more problematic. Possibly my ND tendency to not want to ask for help has also worked to my disadvantage. Despite being registered as a care giver with the GP and Local Carers Support organisation, my entitlement to a carers assessment passed me by. My mother was self-funding, and we were not in direct touch with the social care department. I also did not do the research. My emotions were fully stretched. As a result I missed out on accessing available funding, to cover backfill carers, who could have covered me when I had time away, so that I could have the respite to which I was legally entitled.
In 2021 the care agency we started to use when my mother’s needs increased, persuaded me to book a carer assessment. The conversation focused on things useful to the social care department, such as: lasting power of attorney (which was in place), documentation for my mother’s do not resuscitate order, and her emergency care plan (in case I have an accident). All of which cost social services nothing. The assessor did not mention the ways they could provide me with respite or other support.
In the last year my mother has become entitled to support for her care package, over 9 years she had used up all her savings. The issue of my legal entitlement to respite suddenly became part of the agenda. Possibly because the funding for respite care, came out of a different budget from my mother’s package. The support for me could then be used to offset some of her care costs.
It was frustrating I was not made aware of what I was legally entitled to at a much earlier stage. In many ways this reminded me of the opaque nature of access to work , support for neurodivergent people in employment. Unless you do your research in advance it is very difficult to get the support you need and are entitled to.
4.3) The system is fragmented, despite the best intention of most actors, the interaction of agencies leads to sub optimal outcomes.
My first lecture at the University of East Anglia (back in 1982) was given by Professor Martin Hollis. He introduced me to the concept of Games Theory. Something which has fascinated me ever since. The scenario described in Table 1 is taken from his book Trust within Reason. This Games Theory Puzzle illustrates how rational, well-meaning, professionals, who are loyal to organisational priorities can interact in ways which deliver sub optimal outcomes.
Table 1-Adapted from Trust Within Reason. – Professor Martin Hollis (Hollis, 1998)
This Games-theory scenario is designed to illustrate how under certain circumstances two rational agents with an interest in collaboration may interact with each other in a manner, which is counter-productive to both agents’ interests.

The puzzle is set in a Country Park, which contains a walk, the Enlightenment Trail. The trail climbs a hill, but is punctuated by six pubs. Two walkers, Adam and Eve, have decided to tackle the trail but, being drinkers as much as walkers, they have agreed they will end their walk at one of the pubs. As they reach each pub they will take it in turns to decide whether to halt or continue. Adam will have the first turn.
Neither walker much likes the first pub, The Rational Choice. Adam gives it a score of 1 in his ranking of 5 for the best pub and 0 for the worst, while Eve gives it a score of 0. (Scores are recorded in brackets next to each pub on the above map. Adam’s score is listed first) The next pub, The Social Contract, also scores poorly, (0,2). Then the standard rises; The Foole scores (3,1) and The Sensible Knave (2,4). But the two last pubs are clearly the best on the trail. Adam’s favourite is The Extra Trick, which scores (5,3) while Eve prefers the final pub, The Triumph of Reason (4,5)
Where will the walk end? The enlightened answer should be The Triumph of Reason, the pub that achieves the highest combined score. This however will not necessarily be the case. Adam and Eve symbolise rational organisations with a statutory duty to maximise their own performance. They are also aware their partner is under the same obligation.
The knowledge that both organisations are aware that they will each make rational decisions makes it unlikely that the walk will end at The Triumph of Reason. At the last fork Adam will chose his favourite pub, The Final Trick. However the walk would not progress this far. Knowing Adam’s likely decision Eve would have chosen to end the walk at her second favourite inn, The Sensible Knave. Being under an obligation to act rationally, Adam would be forced to pre-empt Eve’s move by selecting The Foole. Similarly, Eve could not allow this to occur. She would therefore halt the walk at The Social Contract, if she were given the chance, but she would not get the chance. Adam would anticipate the entire chain reaction and end the walk at The Rational Choice. The worst pub of all.
During my time as a care giver, I have often been reminded of this scenario. Many professionals have been involved. GPs, District Nurses, Hospital, Consultants, Social Workers, Physiotherapists , Occupational Therapists and Mental Health Professionals , each well-intentioned but each funded through different channels. The way they interact is complex and often leads to sub optimal outcomes, not only for my mother and I but also for the health and care system.
When my mother was in hospital at the start of 2015, she had three bouts of pneumonia. During the second bout , which occurred the week between Christmas and New Year, the consultant called me and asked me to inform my sisters as he was not sure she would make it. Two days later after my younger sister had flow in from abroad. We were called in to see the same consultant. We were bemused to be told, mum had recovered from her perforated ulcer and we should find a place in a care home and prepare for discharge. The consultant was making a rational, decision, he needed her bed for other patients. It was the middle of winter and lots of people were getting flu. From my perspective my mum was still exceptionally frail , not eating and needed the care she was getting in Hospital. I don’t think the consultant expected her to survive long.
The social care department responded not so fast. No assessment had been made of her care needs . A relative was also able to inform us, about my mothers, right to rehab. After much negotiation, she was transferred to another hospital for rehab. Two months later she was discharged, back to her home where she made a good recovery. During this period the occupational health team who were excellent put in place, a number of adaptations in the home to make it safe.
More recently the social care department has been assessing my mothers care needs. Their first move was to suggest, she should be assessed for continuing health care funding, which would be covered by the national health service rather than the council. My mother had been having problems swallowing. These had been successfully treated by a consultant gastroenterologist who she had been referred to by her GP. The social care department however wanted her to see the speech and language team, as they considered this would lead to her to score more points in the CHC assessment process. Similarly although the GP had fairly successfully treated her agitation , they wanted the mental health team to be involved . Again to score more CHC points. This has all increased worked for other services supporting care, raised my and my mother’s anxiety level and cost the health service more money.
- ND People face additional challenges in navigating the care system.
Many people find the health and social care system hard to navigate. I am aware I have enjoyed many advantages. These advantages include a master’s degree in public policy, family members who have worked in the health sector and others who have provided legal advice to health and care bodies. As well as friends who have experience of negotiating the care maze. I am also not a passive player I am used to taking on authority, rather than accepting the views of professionals. Even with these advantages it’s been hard going.
Access to resources (networks , knowledge and finance) play an important role in securing desired outcomes or at least reducing randomness. This leads to inequalities. Somethings seem to work extremely well for everyone. Other things only work if you are able to fight.
The rules of compound disadvantage apply. A neurodivergent person with access to good networks , knowledge and finance is likely to be at an advantage compared to people with out access to these resources . However an ND person with access to the same resources as an non ND person is likely to be at a disadvantage for some of the following reasons.
5.1) ND people are more vulnerable to trauma anxiety and depression.
Table 2 – The Dyslexia Vortex – Slide from the 8 Ds of Dyslexic well Being (Aston, 2015)
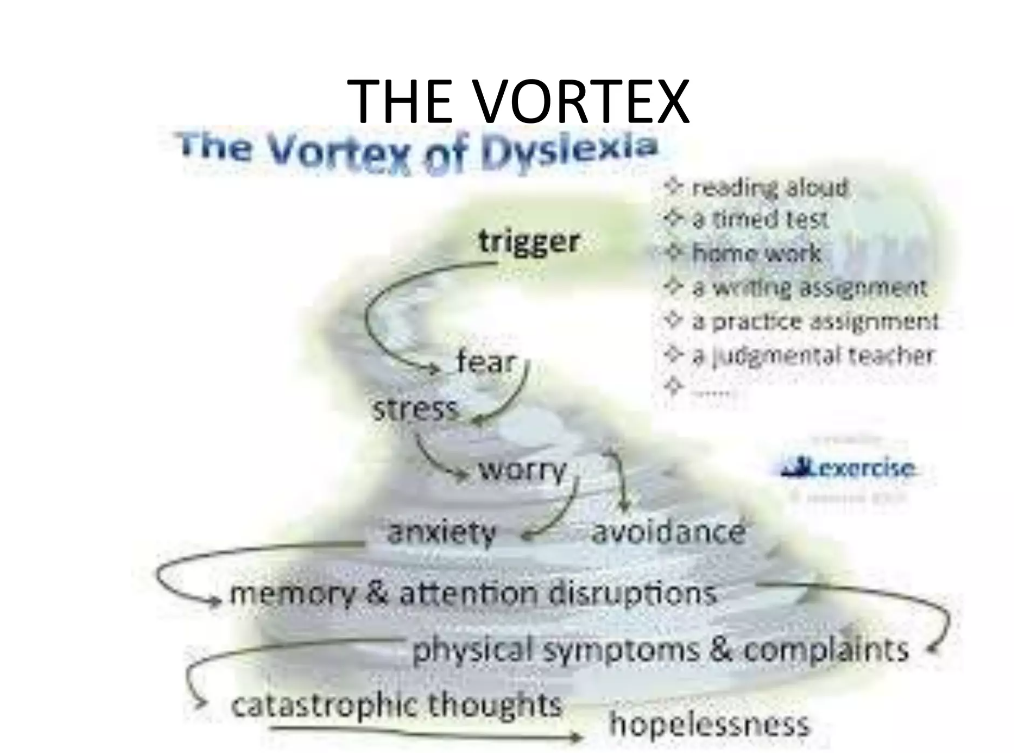 |
Being a care giver can at times be a high stress role. Dr Tony Lloyd Chief Executive of ADHD foundation when commenting on increased demand for ADHD and Autism Diagnosis (LLoyd, 2024) noted that ND people are “more vulnerable to trauma anxiety and depression.
I was made aware of the way encounters in everyday life can set in motion a vortex of negativity during a presentation by Pennie Aston founder of GroOops dyslexia aware counselling.
At times I have undoubtedly felt sucked into this downward negative spiral as a result of encounters with care professionals. An assessment meeting where the social worker declared my mother clearly did not need 1-1 support as her carer had left her alone in her chair, for 30 seconds to let the social worker in through the front door , set the red mist swirling.
When challenged about this statement the social worker could not answer. I asked what the criteria for 1-1 support were, all three of my mother’s falls in last year occurred when she was left alone for less than a minute. The doctor advised someone should be close enough to notice if she was on the move all the time, why did this not qualify as a need for 1-1 support? The front door is in easy earshot of my Mum and 10 strides away, so I did not think opening the door counted as leaving her alone.
I recalled my mother telling me how often teachers and educational psychologists had told her my difficulties at school were the result of her being an anxious parent. When dealing with both care and health professionals I have sometimes been left with the same sense of powerless as I felt as a child. Important professionals making decisions about me and someone I love, without my having much control over the outcome.
5.2) Disclosure frequently does not feel safe.
At work I have always disclosed to my employers at interview that I am Dyslexic and or ND. Sometimes this did not go well. After these bad experiences I have comforted myself in the knowledge that working for someone who had a bad attitude at interview would have been a nightmare.
When dealing with health and social care professionals who have power to make life changing decisions, I don’t want my ND conditions to misconstrued as indicating that I am not competent to make rational decisions or have the capacity to care. Particularly when I don’t feel I can trust them to put my mother’s care needs rather than economics as top priority.
When I have disclosed to some GPs at my local practice and other professionals it has been fine. The reaction of others however has not always been good. Some seem to have a poor understanding of neurodivergence that leads them down a path which end up with them appearing to treat me as sub normal or mentally ill.
I am consequently nervous about what might be on my record, and how that might be interpreted. It also makes me cautious about who I can ask for help. This is not helped by it being difficult to choose which GP, I or my mother get to see when we make an appointment. Building a relationship with a trusted individual is always going to be a challenge given the level turbulence at the local surgery, in the health service and in the social care department.
5.3) Information and Stimulation Overload.
Often the experience of being a care giver is overwhelming. I am fairly sure this is a common experience for everyone not just ND people. Many of the assessment processes are dependent on filling in long detailed forms. These come with detailed written guidance. Stress makes my dyslexic traits more pronounced. Being confronted with these forms, causes me to detect a meltdown could be imminent.
Similarly, the health and social care system is made up of many moving parts. These frequently don’t know much about each other. Researching who you are meant, to contact to get advice or access a particular service, is not easy. For example, who do you call to get authorisation to claim free continence pants, Is it the GP? , is it the district nurse, or is it the social care department. . The answer is It’s the District Nurse, but you can only contact them if the GP makes a request.
5.4) Some assessments and pathways to support rely on a codified scoring system.
It took me a long time to learn, I needed to use key words and evidence skills listed in a person specification, when making job applications. If I did not use the right code, I would not get an interview for a public sector job.
The same type of codification is used in many of the care and medical assessments. The intention is good. Scoring need against set criteria is intended to increase objectivity and make assessment fairer. The code is hidden in plain sight. Detailed guidance documents set out how the process is designed to work. However knowing how the system works and knowing how to fill out the forms to maximise your score, makes it more likely that you will get the outcome which is most beneficial. As an ND person reading guidance and learning how the scoring system works, so as to maximise advantage does not come naturally.
When my mother was having her continuing health care CHC assessment, I was very aware of the codified scoring. I was also aware of the bizarre consequences of the evidencing process. After one fall the ambulance service attended my mother. They were brilliant, they checked her over , were satisfied nothing was broken , and their were no head injuries . They informed us she had a right to go to hospital but there would be a long wait and advised she go back to bed. From my perspective a great outcome. Social Services were however disappointed as if she had gone to hospital this would have increased her CHC score.
The reality was that CHC assessment was extremely well managed by the Nurse from the integrated care board. I don’t think what ever I put in the family statement would have made much difference to the outcome. It was however weird that process was done on line and know one who had actually met my mother had much input.
- Conclusions
6.1) Neurodivergence Impacts on all Aspects of life .
My experience as a care giver has reminded me that my neurodivergence impacts on all aspects of my life. Sometimes it’s a strength sometimes it’s a weakness but it’s always there. Much of the mainstream discussion about neurodivergence focuses on education and employment. Putting in place support to help us pass exams, get work and stay in work. This is obviously important. Life is however about much more than exams and work.
Neurodivergence impacts on our family relationships. Our ability to access support systems including public services, such as health and social care. Our ability to enjoy ourselves and engage in meaningful activity. For me this is frequently sport and physical exercise. One of the reasons I so enjoy my engagement with Neurodiverse Sport.
6.2) My experiences as an ND person navigating the health and social care system, is the same as everyone else’s, but with ND spice.
Prior to engaging with the ND community and becoming ND aware. I would have ignored the impact of my neurodivergence on my experiences in navigating the care system. I would have assumed my experience was just the same as everyone else’s. Mostly this would have been correct. I am getting the same service as everyone else. Not only ND carer givers get the blues .
Because I am aware of my neurodivergence, I am conscious that at times I have hit information overload and that I have been triggered by some of my encounters. This awareness is a protection factor. It gives me a clue as to why at times I react, in a disproportionate way.
6.3) Public Services Need to be more aware that at least 15-20% of users are ND .
Public services, not just health and adult care but housing, benefits, job centres and young people’s services, by their nature provide a safety net for people facing challenges. It is therefore likely a disproportionate number of service users will be ND. The department for Justice has in recent years become aware that ND people are over represented in the Justice System. The Department for Justice has therefore produced a neurodiversity action plan. By the end of 2024 every prison will have a neurodiversity managers as will many probation services. (Group, 2023)
I wonder if a similar model could work in the health and social care world? Could the infrastructure provided by carers uk and the local carer support organisations , include an ND advice point. This might provide advice at arm’s length from clinical or social work professionals. Could more be done to make GPs and other health and social care gatekeepers aware of the needs of often undiagnosed ND service users.
One step might be to consider a universal design approach, Frequently care givers are not good at assessing their own needs . A possible answer would be, any one registered with the GP as a Care giver should automatically have appointments (perhaps 6 monthly) , with a care advice professional . These would track the level of pressure and check all entitlements to support, carers allowance , respite and council tax reductions were being accessed. This is probably the intention of carer reviews. However the current system is not working , as it requires the carer to be proactive and is not automatic . The assessor are also not independent and have an interest in limiting the level of support some carers access.
6.4) Carer Wellbeing is Key not just for ND People
Politicians and the Media like to draw attention to the fact that unpaid care givers save the NHS billions. To do this they need to remain both physically and mentally healthy. Carer Wellbeing is key to stopping this system collapsing.
I accept some of this is a personal responsibility. On many occasions I have found the wheel of wellbeing a useful tool to gauge how I am feeling, and to identify some of the factors that I need to ensure are in place if I am to maintain my mental health. I am fortunate to have family support , to still be able to do some interesting work , to play tennis regularly and to be fairly financially secure .
The Wheel of Wellbeing

Care giving for an aging relative inevitably mostly points to a certain outcome. The path towards that outcome contains some highs as well as lows. At the low points I have been disappointed that this system is not equipped to factor in support for caregiver wellbeing.
When my Mum was admitted to hospital in 2014, with her perforated ulcer . The Anesthetist was fairly blunt that her chances of survival were better than 50:50 but not much. The honesty was welcome but it comes with no after care, which can make it difficult for families.
When my Mum got her diagnosis of vascular dementia in 2021, I would have welcomed someone checking in on me to ask , how I was coping and to explain what to expect . The professional focus was all on the patient and not on the care giver. Although I was given a huge pack of leaflets , I did not want reading material.
When I have received support it has been because , occasionally professionals have stepped outside their job roles to offer amazing kindness . Just before Christmas in 2014 , while my mother had her first bout of Pneumonia, a nurse told me her body was shutting down . I called my sister and asked if the hospital offered a counselling service for people facing bereavement . They didn’t but a young Indian junior doctor on her break, said she would sit with me until my sister arrived. It made a huge difference . As it happens after an hour I went back in to ITU . antibiotics started to kick in, and my mother recovered.
Works Cited
Aston, P. (2015). the 8 ds of dyslexia wellbeing . Retrieved from Slide Share : https://www.slideshare.net/RuthEllenHenryOvidMI/gro-oops-dyslexic-wellbeing-the-8-ds
Careruk. (2024). Key facts and figures about caring . Retrieved from Careruk : https://www.carersuk.org/policy-and-research/key-facts-and-figures/
Ekinsmyth, C. (2013). Mothers’ business, work/life and the politics of ‘mumpreneurship’. Retrieved from Researchgate: https://www.researchgate.net/publication/267153766_Mothers’_business_worklife_and_the_politics_of_’mumpreneurship’
Freeman, C. (2023, October ). Economics of Neurodiversity 2 – Employment and Unemployment . Retrieved from Charles Freeman Projects : https://charlesfreemanprojects.com/about-neurodiversity-economics/
Gov.uk . (2024). https://www.gov.uk/carers-allowance/eligibility. Retrieved from Gov.UK: https://www.gov.uk/carers-allowance/eligibility
Group, W. f. (2023). Neurodiversity Action Plan Update. Retrieved from HM Gov Media Services: https://assets.publishing.service.gov.uk/media/63d0026b8fa8f53fe41ff691/NAP-Update-2023-final_proof_25012023.pdf
Hollis, P. M. (1998). Trust Within Reason . Cambridge University Press.
Kirby, P. A. (2021, June ). Neurodiversity 101 Hereditability. Retrieved from X formerly Twitter : https://twitter.com/profamandakirby/status/1399972576659705856?lang=en
LLoyd, D. T. (2024, April 04). ADHD and Autism Diagnosis . (B. b. https://www.linkedin.com/posts/jennie-meadows-photographer-and-artist_the-sudden-rise-of-audhd-what-is-behind-activity-7181543695689625600-z9wu?utm_source=share&utm_medium=member_desktop), Interviewer)
NICE. (2024). Glossery. Retrieved from NICE: https://www.nice.org.uk/glossary?letter=q#:~:text=Quality%2Dadjusted%20life%20year,-A%20measure%20of&text=QALYs%20are%20calculated%20by%20estimating,a%200%20to%201%20scale).

I am an experienced policy researcher and strategist, specialising in Culture Sport and The Creative Economy.
I started my career as researcher for a Tourism and Regeneration Consultancy. I then worked in Higher Education and Local Government, before Joining Sport England.
I worked to embed the interests of the Department for Culture, Media and Sport (DCMS) sector within regional policy as Executive Director of Culture South East.
I am currently a Director of my own company . Recent projects have focused on The Creative Economy, Place Shaping, Cultural Planning and Employability.
I am Neurodivergent (Dyslexic and Dyspraxic) and have a particular interest, in Neurodivergence in the Creative Economy, Including, Employment and Self Employment.